Bring to the table win-win survival strategies to ensure proactive domination. At the end of the day, going forward, a new normal that has evolved from generation.
Lorem ipsum dolor sit amet, consectetuer adipiscing elit, sed diam nonummy nibh euismod tincidunt ut laoreet dolore magna. Ut wisi enim ad minim veniam, quis nostrud exerci tation ullamcorper suscipit lobortis nisl ut aliquip ex. Duis autem vel eum iriure dolor in hendrerit in vulputate velit esse molestie consequat.
CERVICAL CANCER SCREENING – WHY YOU MUST GET SCREENED EARLY!
By Zaynab Solahudeen
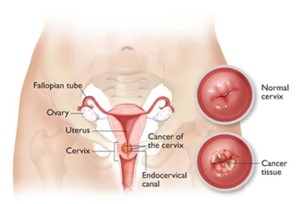
It is quite common: Cervical cancer is the fourth leading type of cancer among women globally, with roughly 604,000 new cases and 342,000 deaths in 2020, where majority of the new cases and deaths in 2020 occurred in low- and middle-income countries (GLOBOCAN). It is now considered to be a sexually transmitted infectious disease that is caused by a persistent infection of the lining of the cervix (a canal that connects the uterus and vagina), by Human Papillomavirus (HPV). HPV types 16 and 18 are more common.
The Cervix – Normal & Diseased Source: BusinessMirror
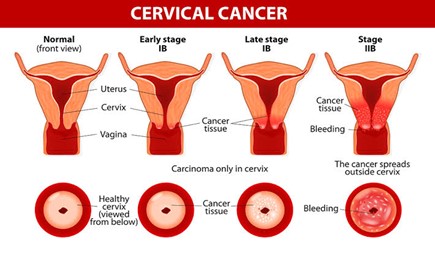
How you get it: It is commonly spread through sexual contact with an HPV infected person. A sexually active person is therefore more likely to get infected. Although a transient infection can resolve spontaneously, persistent infection that is not detected for appropriate treatment can predispose you to developing frank cervical cancer in later years. It takes 15-20 years for the cancer to develop after infection, but in HIV infected persons, the period is shorter, it takes about 5-6 years to manifest. HPV causes the normal cells of the cervix to transform into abnormal cells which eventually becomes cancer, and the cancer can spread to involve nearby organs such as the womb, pelvis, urinary tract, and other organs of the body.
Progression of Cervical Cancer Source: drandreworr.com
To avoid getting cervical cancer: The only way is prevention. Cervical cancer can arise from any kind of unprotected sex from an infected person. Men can be carriers of HPV and pass it on to their sexual partners. Most sexually active adults may have HPV infection and will be totally unaware of this infection until a screening is carried out. The primary screening test recommended by the World Health Organization is the HPV DNA Test, which is available to only women. There’s currently no approved test for detecting HPV in men.
Screening: It is highly recommended for every woman of sexual and reproductive age, to get screened routinely every five years for cervical cancer, irrespective of their age.
Vaccination:Gardasil and Cervarix are the two approved HPV vaccines and can be used for both genders. It is given before both boys and girls are exposed to the virus between the ages of 11 and 12, or as early as 9 years of age. The Centre for Disease Control (CDC) recommends that young adolescents (9-12 years of age) and teens receive two doses of the vaccine at least 6 months apart. However, teens and young adults between the ages of 15-26, should receive three doses of the vaccine.
Practice Safe Sex: Having multiple sexual partners and not using a condom puts you at a very high risk of contracting an HPV infection. It can also lead to having other sexually transmitted infections like Chlamydia and Gonorrhoea which can further depress your immune system making it harder to deal with an HPV infection and posing a faster rate to developing cervical cancer.
Smoking: Cigarette smoking increases the risk of developing any form of cancer, and cervical cancer is not an exception.
If you have ever had a Pap smear for cervical cancer screening, you should thank George. George Papanicolaou.
George Papanicolaou (13 May 1883 to 19 February 1962) is the inventor of Pap (short for Papanicolaou) smears. He first reported that uterine cancer cells could be detected in vaginal smears in 1928. “The first observation of cancer cells in the smear of the uterine cervix” he later wrote, “gave me one of the greatest thrills I ever experienced during my scientific career.”
Cervical cancer is the second most common cancer among women in Nigeria. It is sad, seeing that this is a hugely preventable disease. A Pap smear can detect early signs of cervical cancer. It takes less than five minutes to be done and the results are ready in a couple of days. A pap smear should be done every three years if previous results have been normal.
A Spatula and glass slide. Instruments used in the Pap smear.
A microscopic picture of normal cervical cells
A microscopic picture of abnormal cervical cells
You should have a pap smear if you are having sex (single/multiple partner) and over 25 years of age.
At The Specialist Laboratories we provide a private, confidential and conducive environment for all investigations including the pap smear. Home/office tests are also available on request. Our team of specialists have over fifty years of combined cervical cancer screening experience.
A Pap smear is just a call away. Contact Dr. Nnamdi on 08022289151 for more information or fill this form and a representative will get across to you.
Why the LBC/HPV CO-TEST is the preferred screening method.
Cervical cancer screening is the process of detecting and removing abnormal cells in the cervix before cervical cancer develops. Screening methods include:
Pap test (also known as Pap smear)
Liquid Based Cytology (LBC)
Human Papillomavirus (HPV) DNA testing
Visual inspection with acetic acid (VIAA)
HPV RNA TestingPap Smear
The Pap smear is done by collecting cells from the cervix and smearing them on a glass slide. This method is fraught with errors of collection and analysis as there is a large amout of debris admixed with the cells of the cervix thereby hampering interpretation.
The LBC is an improvement on the Pap smear. The cervical cells are collected in a liquid vial and then spun to remove the accompanying debris. The liquid can also be used for HPV testing.
HPV testing is the gold standard for screening. HPV is the causative agent of cervical cancer. This test detects the presence of HPV infected cells in the cervix. It can also specify if the HPV strain is low or high risk.
VIAA is done by smearing the cervix with acetic acid and visually observing the colour changes that result. A huge disadvantage of this method is that inflammation and atrophy could mimic cancerous changes and result in over-treatment of the patient.
Why is the HPV/LBC CO-TEST the preferred screening method?
The LBC test can be prone to false negatives and false positives. This is due to anatomic changes in the cell for example in atrophy and inflammation. It cannot reliably detect the presence of HPV The HPV test can detect the presence of HPV but the presence of HPV does not imply that there are pre-neoplastic changes present. It is known that HPV infections can be cleared by the body’s own immune system and therefore the presence of HPV does not indicate a certain progression to cervical cancer. The purpose, then, of the HPV/LBC co-test is to merge the strengths of the two screening tests to derive maximum benefit. The HPV test detects the presence (or absence) of HPV in the cells and if they are high risk strains. If high risk strains are present, the LBC test then looks for changes in the morphology of the cells indicating a progression to cancer. In other words, the HPV test acts as a triage before the LBC test making it a cost-effective screening measure.
The HPV/LBC co-test is to be repeated every five years and so is more convenient.
At The Specialist Laboratories, the HPV/LBC co-test is done in a licensed laboratory by our trained scientists and consultants.
Hormone receptor profiling is necessary for breast cancer treatment. Just as no two people are exactly alike, no two breast cancers are exactly the same, either. The pathology report contains certain pertinent information including:
At TSL, we use a synoptic reporting template which ensures that all our reports are standardised and can be used worldwide. The breast biopsy/mastectomy report is available for download/pick-up/delivery within five working days. This is followed by ER, PR and HER2 analysis on request.
IHC Machine
We provide in-house automated immunohistochemistry for hormone receptor (ER, PR) analysis and HER2 testing as well as partnerships with overseas laboratories to provide FISH testing for indeterminate HER2 cancers. Hormone receptor analysis reports are available within 2 weeks. We also offer Oncotype DX testing to help you make a more informed decision on treatment for ER positive breast cancers.
You want to give the best treatment to your client/patient diagnosed with lung cancer but you are at sea concerning how to go about it. Read on to find out more.
Targeted therapies guided by molecular diagnostics have become a standard treatment of lung cancer. Epidermal growth factor receptor (EGFR) mutations and anaplastic lymphoma kinase (ALK) rearrangements are currently used as the best predictive biomarkers for EGFR tyrosine kinase inhibitors and ALK inhibitors, respectively.
Indications for molecular testing.
The important reason for molecular testing of lung cancers is to select patients who may benefit from targeted therapies. In addition, patients with lung cancer can get benefits from molecular testing of their tumors regardless of stage. For example, molecular testing can provide accurate information on staging (in case of multiple tumors), prognostic stratification, and prompt treatment in case of recurrence. Because of the high frequency of EGFR mutations in Asian populations as mentioned above, EGFR mutation testing is especially important for the treatment of Korean lung cancer patients. Other mutations can also be approved and used as predictive markers in the near future. Each mutation is significantly associated with some clinical factors or histological subtypes.
Positive ALK-FISH test
Nevertheless, clinical findings alone cannot completely predict specific mutation status. In most of the guidelines published so far, histological types have been recommended as the most important factor in determining whether to perform molecular tests. In particular, for patients who have a diagnosis of non- small cell lung carcinoma (NSCLC) with an adenocarcinoma component or non-squamous cell type, molecular testing is routinely recommended. Thus, pathologists should try to further classify NSCLCs into more specific subtypes, such as adenocarcinoma or squamous cell carcinoma (SQC). Besides histological analysis, in cases of young age, female gender, never-smokers, small biopsies, or patients with a combined tumor type, molecular testing can be done.
Immunohistochemistry for Lung Cancer
Procedure
Formalin-fixed, paraffin-embedded (FFPE) tissues are most frequently used in molecular testing. Routinely prepared FFPE tissues are the most practical resource for molecular analysis, in spite of fixation-related artifacts. The optimal fixative for preparing FFPE samples is generally 10% neutral-buffered formalin. The optimal fixation time ranges from 6 to 72 hours to avoid underfixation or overfixation, respectively. Routinely prepared cytology samples such as alcohol-fixed smears or Thin Prep slides and cell block samples are also suitable for mutation testing.
Sample requirements
The presence of tumor cells in a sample must be confirmed before mutation analysis. The percentage and quality of tumor cells are crucial for proper mutation testing. For example, direct sequencing requires at least 20% tumor cells in the sample for reliable testing result.
Methodology
At TSL, lung biopsy samples are processed and histology reports are given within 5 working days following which molecular testing is done if requested for. EGFR testing is done by PCR, ALK by immunohistochemistry and FISH while PD-L1 is done by immunohistochemistry. Molecular testing reports are usually available within two weeks.
The last week in April is set aside worldwide to commemorate ‘world vaccination week’. At the mention of the word ‘vaccine’, I immediately begin to think of vaccine-preventable childhood diseases. I am pretty certain that most of us have memories of being vaccinated in school or have seen children being vaccinated. We rarely think of adult vaccinations most especially the Human Papillomavirus (HPV) vaccine. The high-risk Human Papillomavirus (HPV) serotypes are the causative agents of cervical cancer and have been implicated in the causation of penile cancer, anal cancer and oropharyngeal cancer. There are about 16 high-risk serotypes of HPV including types 16, 18, 33, 35, 52 and 56. About 3.5% of women in the general population are estimated to harbor cervical HPV-16/18 infection at a given time, and 66.9% of invasive cervical cancers are attributed to HPVs 16 or 18. The virus can be transmitted from an infected person through unprotected sexual intercourse, genital-to-genital rubbing, oral sex and anal sex. Cervical cancer is the second most common cancer among women in Nigeria today. Current estimates indicate that every year 14943 women are diagnosed with cervical cancer and 10403 die from the disease. Cervical cancer ranks as the 2nd most frequent cancer among women in Nigeria and the 2nd most frequent cancer among women between 15 and 44 years of age HPV infection is preventable through the use of vaccines. The vaccine is recommended for adolescents who have not been exposed to sexual intercourse. The bivalent vaccine protects from types 16 and 18. However, the individual may be infected by other serotypes. Routine screening is essential for detecting early changes in the cell which could signal later development of cervical cancer. Pap smears can be done every three years and HPV screening done every five years.
Dolor sit amet, consectetuer adipiscing elit, sed diam nonummy nibh euismod tincidunt ut laoreet dolore magna aliquam erat volutpat. Sed fringilla mauris sit amet nibh. Donec sodales sagittis magna. Sed consequat, leo eget bibendum sodales, augue velit cursus nunc, sapien ut libero venenatis faucibus.
Dolor sit amet, consectetuer adipiscing elit, sed diam nonummy nibh euismod tincidunt ut laoreet dolore magna aliquam erat volutpat. Sed fringilla mauris sit amet nibh. Donec sodales sagittis magna. Sed consequat, leo eget bibendum sodales, augue velit cursus nunc, sapien ut libero venenatis faucibus.
Quis tibi ergo istud dabit praeter Pyrrhonem, Aristonem eorumve similes, quos tu non probas? Quoniam, si dis placet, ab Epicuro. tiam rhoncus. Maecenas tempus, tellus eget condimentum rhoncus, sem quam semper libero, sit amet adipiscing sem neque sed ipsum. Nam quam nunc, blandit vel, luctus pulvinar, hendrerit id, lorem.
Dolor sit amet, consectetuer adipiscing elit, sed diam nonummy nibh euismod tincidunt ut laoreet dolore magna aliquam erat volutpat. Sed fringilla mauris sit amet nibh. Donec sodales sagittis magna. Sed consequat, leo eget bibendum sodales, augue velit cursus nunc, sapien ut libero venenatis faucibus.